Each month, our team at Lightning Dental Charts reviews rulings and case discussions from the Dental Board to identify emerging themes in clinical judgment, documentation, and risk management.
April’s Board meeting contained a larger number of instructive cases than usual, so we will be splitting this month’s analysis into two separate posts. Part I focuses on two recurring themes that appear frequently in Board investigations: informed consent documentation and how dentists should chart complications when treatment does not go as planned.
1. Crown Deliveries, Informed Consent, and What Must Still Be Documented
The first case involved a single crown. The patient later filed a complaint, and one issue reviewed by the Board was the absence of a signed consent form.
The Board ultimately held that delivery of a single crown does not necessarily require a separate written consent form. However, the progress notes still needed to reflect that the dentist discussed the advantages, disadvantages, risks, and alternatives (ADRA) with the patient and that the patient accepted treatment.
Many dentists assume informed consent is an all or nothing issue tied exclusively to signed forms. In reality, Boards may also evaluate whether the chart itself demonstrates that an informed discussion occurred, even when no standalone consent document is required.
From a documentation standpoint, crown cases should generally reflect:
- The restorative options discussed
- Risks and limitations of treatment
- Alternatives such as extraction or no treatment
- The patient’s acceptance of the proposed plan
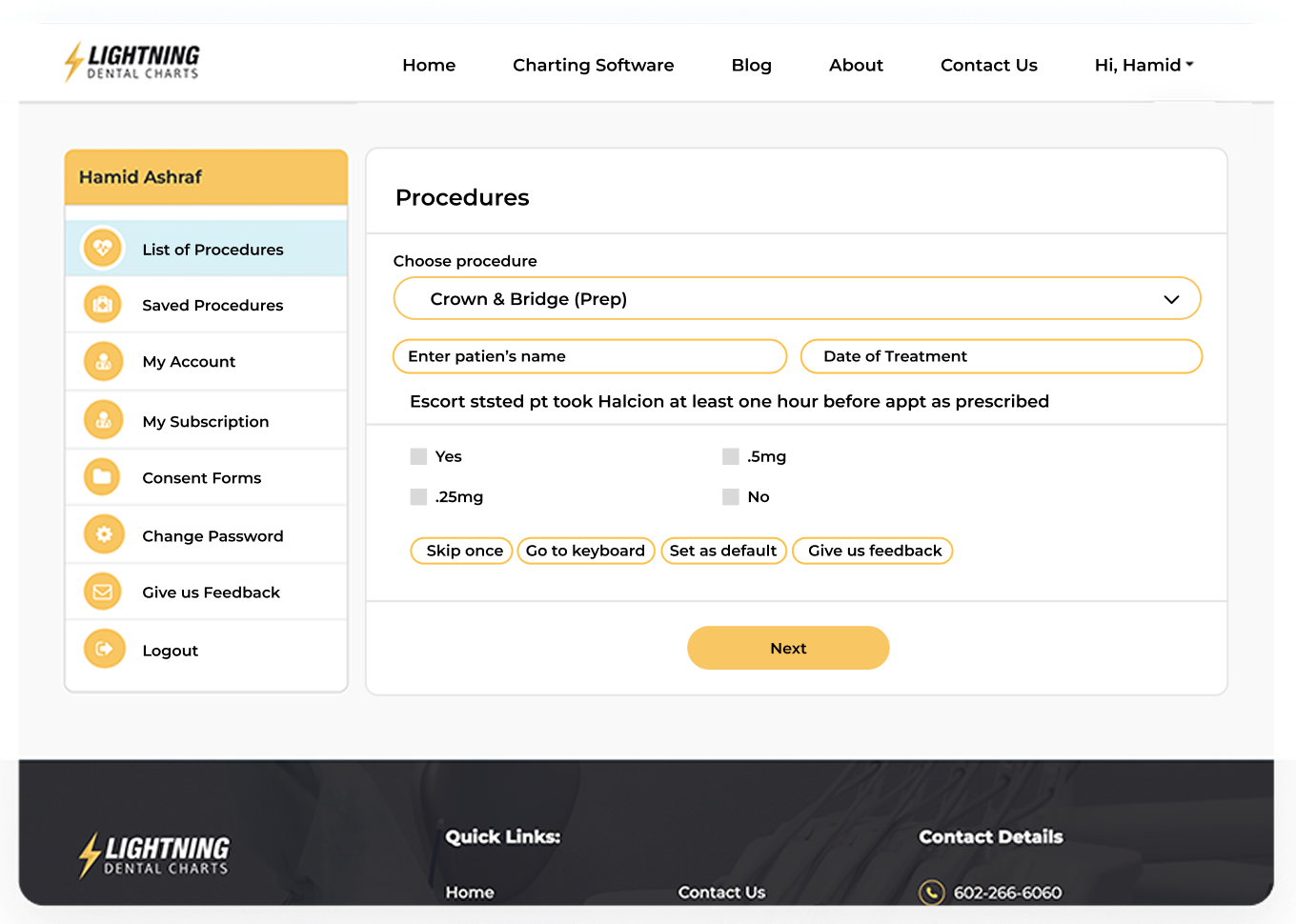
This is one reason Lightning Dental Charts uses structured prompts that document advantages, disadvantages, risks, and alternatives directly inside the progress note workflow. The system also includes dedicated consent forms for crown and bridge procedures when practices prefer additional written protection.
The broader takeaway is straightforward: even relatively routine restorative procedures can create Board exposure when the chart does not clearly reflect the informed consent discussion behind the treatment.
2. Retained Root Tips and How to Chart Complications Correctly
Another April case involved retained root tips following an extraction. The dentist sectioned tooth #18 and reassembled the extracted portions on the tray to confirm removal. Despite those efforts, two small root tips remained. The patient later developed an infection that ultimately required emergency room treatment.
The Board held that a post-extraction confirmatory PA is not necessarily the standard of care. It also reaffirmed that known retained root tips measuring 2 mm or less may be left intentionally when anatomical concerns justify doing so, provided the reasoning is properly documented.
This case highlights an important principle that extends far beyond extractions.
When complications or unexpected outcomes occur, the chart must establish three things clearly:
- The dentist recognized the complication
- The patient was informed
- A contingency plan was discussed and accepted
In cases involving retained root tips, documentation should explain why retrieval was not attempted, the risks discussed with the patient, and the follow-up plan moving forward. An example of a defensible entry might read:
“Post-extraction PA reveals two 2 mm root tips remain. Retrieval not attempted due to inferior alveolar nerve (IAN) proximity. Patient informed of retained root tips and associated risks. Area to be monitored at future hygiene and periodontal maintenance visits. Patient instructed to call immediately if symptoms develop and oral surgery referral discussed if complications arise.”
The key issue is not whether a complication occurred. The key issue is whether the chart demonstrates recognition, communication, and appropriate follow-through once the complication became known.
Final Thoughts
April’s first set of cases reinforces a recurring theme in Board investigations.
Many complaints do not arise because the dentist ignored the issue. They arise because the chart failed to demonstrate that the dentist recognized the issue, discussed it appropriately, and created a reasonable plan moving forward.
Clear documentation remains one of the strongest protections a dentist has when treatment outcomes become unpredictable.
Lightning Dental Charts is designed to help practices create thorough, defensible records efficiently through structured prompts, informed consent workflows, and documentation safeguards that align with how Boards actually review cases. If you would like to strengthen your documentation workflow while reducing legal exposure and saving time charting, explore Lightning Dental Charts with our 14 day free trial.